



Minor & major surgery (Impaction, cyst removed, sinus lifting)
Impaction




The last teeth to develop and erupt into the jaws are called the third molars. Third molars usually erupt in the late teen years, which coincides with passage into adulthood and is referred to by some as the age of wisdom; hence “wisdom teeth”.Wisdom teeth used to serve a useful purpose, but are now considered vestigial organs. A vestige is a degenerative or imperfectly formed organ or structure which no longer performs a useful function. Wisdom teeth have become “outdated” for many reasons. Our ancestors’ diet was made up of far coarser food than our own and a lack of hygiene meant that impurities such as dirt and sand were consumed regularly. This caused teeth to abrade significantly which meant they took up less space in the jaw. Permanent teeth were also frequently lost at an early age, which would create more space in the jaw. Due to the coarseness of the food it was harder to chew and the jaw itself would develop into a larger bone as it was working much harder. All of these factors would create more space for the wisdom teeth when they came in.
Unfortunately, the wisdom teeth are now usually trying to erupt into a jaw that is too small. The heavily processed diet of today does not produce the tooth abrasion or jaw development that we used to see. Modern dentistry has pretty much eliminated significant loss of permanent teeth at an early age. This leaves us with too many teeth and not enough jaw.
Wisdom teeth serve no useful function and will often cause damage because when a wisdom tooth becomes partially exposed through the gums it cannot be cleaned properly and can collect food debris, bacteria and plaque around itself. This can result in tooth decay, gum disease, infection and abscess of not only the wisdom teeth, but of the nearby molars and surrounding gum tissue. The molars in front of the wisdom teeth are sometimes lost because of cavities and gum disease caused by the inability to clean the wisdom teeth properly. Cyst formation and other destructive pathology are also seen around impacted wisdom teeth. There may be pain and swelling, or you may have no symptoms at all, even though the other teeth in your mouth may be at risk of damage.
If removal of the wisdom teeth is necessary, the procedure is recommended in the late teenage years, before the roots are completely formed. Surgical procedures in general are better tolerated when one is young and healthy, and the gum tissues tend to heal better and more predictably when young. Most people experience minimal disruption of their normal routines, and time off from work or school is usually minimal. At this point it is worth noting that the removal of wisdom teeth can be of great benefit to your ultimate oral and general health.
Wisdom teeth can be extremely problematic and more often than not I advise patients to have their wisdom teeth removed. However, not everyone has problems with their wisdom teeth. If you’re genetically lucky, the jaws are long enough to accommodate the wisdom teeth in a proper erupted position. In this position, if they can be kept clean, they may be used.
How and where your wisdom teeth are removed depends on whether your wisdom teeth are erupted or impacted and how deep the roots are. Surgery may take place in your dentist’s or oral surgeon’s office rather than in a surgical center or hospital. Your dentist or oral surgeon will review the recommended procedure with you so that you are comfortable with the procedure from the very beginning. You will also be given information about eating, medication, rest, driving, and other considerations for the periods before and after surgery.
Immediately after surgery your body sends blood to nourish the tooth socket and the healing process begins. Simple pressure from a piece of gauze should control the bleeding and help a blood clot to form in the socket. After surgery, you will rest while under close observation as you recover from the anesthetic. Once your doctor is satisfied with your recovery you will be able to go home and relax. Within a day or two, soft tissue begins to fill in the socket, aided by the blood clot. In time, the bone surrounding the socket begins to grow, eventually filling in the socket completely.
It is possible for you to heal more quickly and avoid complications by simply following the instructions that your dentist or oral surgeon gives you. However, if you experience excessive bleeding or swelling, persistent and severe pain, fever, or if you experience any reaction to medications, please do not hesitate to call your dentist for further advice. A follow-up examination may also be scheduled to make sure that the socket is healing properly and that your mouth is returning to a normal, healthy state.
Sinus lifting
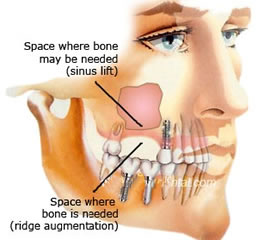
A sinus lift (a sinus augmentation) is surgery that adds bone to your upper jaw in the area of your molars and premolars to make it taller. The bone is added between your jaw and the maxillary sinuses, which are on either side of your nose. To make room for the bone, the sinus membrane has to be moved upward, or “lifted.” A sinus lift usually is done by an oral and maxillofacial surgeon or a periodontist.
It can happen that there is no longer enough bone in the molar area of the maxilla in the direction of the floor of the sinus because of the bone atrophy after tooth loss. As bone augmentation in this region is possible only with difficulty, a method was developed in which the floor of the sinus is raised and bone is inserted into the cavity produced, without injuring the mucosa of the sinus, which leads to an effective increase in the bone in the molar maxillary region. This operation is called a sinus lift. This operation can be carried out under local anaesthesia and is done through the mouth so that there are no scars on the face. The sinus lift operation can often be done at the same time as the insertion of dental implants. The bone material which is inserted corresponds to that described already for bone augmentation.
A sinus lift is done when there is not enough bone in the upper jaw, or the sinuses are too close to the jaw, for dental implants to be placed. There are several reasons for this:
- Many people who have lost teeth in their upper jaw — particularly the molars teeth — do not have enough bone for implants to be placed. Because of the anatomy of the skull, the back of the upper jaw has less bone than the lower jaw.
- Once teeth are gone, bone begins to be resorbed (absorbed back into the body). If teeth have been missing for a long time, there often is not enough bone left to place implants.
- The maxillary sinus may be too close to the upper jaw for implants to be placed. The shape and the size of this sinus varies among individuals. In addition, the sinus can get larger as you age.
- Bone may have been lost because of periodontal (gum) disease.
Dental implants have gained popularity for treating edentulism, but some patients develop jaw atrophy, which leaves insufficient bone for implants. To treat these patients, the sinus lift procedure, which augments bone, was developed. Altered anatomy from this procedure has an unusual radiographic appearance, confusing those unfamiliar with it. We describe the sinus lift procedure and its radiographic appearance.
Procedure
The oral surgeon will cut the gum tissue near your premolars and molars. The tissue is raised, exposing the bone. A small, oval window is opened in the bone. The membrane lining the sinus on the other side of the window separates your sinus from your jaw. This membrane is gently pushed up and away from your jaw. Granules of bone-graft material are then packed into the space where the sinus was. The amount of bone used will vary, but usually several millimeters of bone is added above the jaw.
Once the bone is in place, the tissue is stitched closed. Your implants will be placed four to nine months later, depending on the graft material that was used. This allows time for the grafted material to mesh with your bone.